WHAT IS IT?
Myositis ossificans (MO) is a condition where bone tissue forms within a muscle after injury. Damage of muscle tissue results in bleeding and inflammation within the first 24-48 hours post injury, and within the first week collagen fibres are laid down to repair the damaged tissue. Normally this process takes between 4-6 weeks to complete. With MO, fibrotic tissue is laid down in the muscle, which becomes ossified or calcified tissue.
This results in a hard, palpable lump in the muscle belly, restricted range of motion and reduced strength of the muscle. Unlike an uncomplicated muscle strain, MO can take months to years for the ossified portion to completely reabsorb. Return of muscle function is very dependable on the size of the ossification.
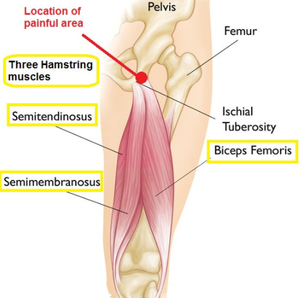
It is most common in the quadriceps, hamstring and back muscles.
HOW DOES IT HAPPEN?
The most common cause of myositis ossificans is significant, direct trauma to the muscle. It is most common in contact sports, however sports such as hockey and cricket also have a high prominence due to contact from the ball. It can also occur after a muscle strain.
You have increased risk of developing MO if you continue playing after a muscle injury, aggressively stretch or massage a muscle injury within the first 48 hours or re-injure the same area.
WHAT ELSE COULD IT BE?
A thorough clinical assessment will rule out any differential diagnosis however, particularly with a history of trauma, MO is hard to miss.
Medical imaging may be useful, however is not necessary to confirm a diagnosis. Ossified tissue can be seen on X-ray after 6 weeks, however if the injury is acute an ultrasound may be used to assess the extent of any haematoma.
Potential differential diagnosis that should be negated by your clinician are:
- Muscle strain
- Muscle contusion/haemotoma
- Joint sprain
- Compartment syndrome
HOW LONG WILL IT TAKE TO GET BETTER?
Over time, the ossification is gradually reabsorbed, however this process may take a number of months. In some cases the ossified growth may never completely reabsorb. This may result in tightness or discomfort when stretching the muscle, however normally won’t impair function of the muscle.
Here are some tips for the duration of your recovery. Your physiotherapist will guide you through an individual rehabilitation program.
Ice/compression
As with most acute injuries, the ‘RICE’ principle should be applied over the first 48 hours. This refers to rest, ice, compression and elevation. Compression can be applied with a tubigrip bandage, and icing for no longer than 20 minutes at a time, with a 2 hours break between ice packs.
Hirudoid cream
Hirudoid cream or gel dissolves small blood clots and reduces inflammation of the affected area. Depending on the area, the cream can be applied overnight and wrapped in gladwrap. It is advised to discuss with your pharmacist or GP before using this medication.
Load Management
Depending on the location and size of injury, you will need to de-load the area for a period of time. If you have significant discomfort walking, you may require crutches for the first few days, before you can tolerate putting weight on your leg. Your physio will then guide you through a program progressing through range of motion, strength, flexibility and power exercises. Unlike a muscle strain, it is okay (and often necessary) to push through slight discomfort with these exercises to regain full range and power of the muscle.
Stretching
An ossified section of the muscle tissue should be vigorously stretched so to not loose length of the affected muscle. Stretching should be performed for 2-3 minutes at a time, multiple times throughout the day. Note that stretching should not be performed within the first two weeks of a muscle injury as it can increase bleeding and should only be performed once the diagnosis of myositis ossificans is confirmed.
Returning to Play
Your physiotherapist should have a strict return to play criteria to ensure there is little risk of re-injury to the area. In contact sports you can play with padding over the area, to distribute the force of subsequent contact. It is oaky to return to play without complete reabsorption of the ossified area, as long are you have met the return to play criteria.
WHAT ELSE COULD I DO?
Anti-inflammatories may be indicated to help the body reabsorb ossified tissue. Your physiotherapist may refer you to a GP or sports physician to prescribe appropriate anti-inflammatories.
Surgical removal of the ossification is rare, and will only occur in those cases near a muscle insertion, where joint function is impaired. Surgery is only performed at least 12 months post original injury.
If you suspect myositis ossificans, your physiotherapist will help you develop a suitable management plan